Imaging findings of perineural spread as mentioned before can be very subtle.
Pay attention to:
- Obliteration of fat planes (on CT and MRI)
- Enlargement of the affected nerve (on MRI)
- Excessive enhancement (on MRI)
- Enlargement of the affected foramen (on CT)
Be aware that apart from intracranially,
the surrounding venous plexus and perineural tissue may enhance physiologically.
It is important to compare it with the contralateral side to detect pathological enhancement.
Normal Anatomy:
Trigeminal nerve:
The trigeminal nerve is the thickest cranial nerve which leaves the pons in a rather lateral position.
It courses straight through the pre-pontine cistern to enter the Gasserian ganglion.

Fig. 2: Illustration of the proximal trogeminal nerve
References: Leblanc
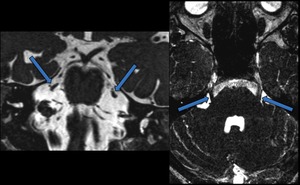
Fig. 3: Coronal (left) and axial (right) CISS
The arrows depict the trigeminal nerve in the pre-pontine cistern
Coursing ventraly the third division of the trigeminal nerve (maxillary branch) is the first one to exit the skull through the foramen ovale.
The first branch (ophtalmic/ V1) and the second branch (mandibular/V2) course through the cavernous sinus.
The first then courses through the superior orbital fissure; the second through the foramen rotundum.
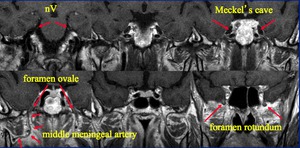
Fig. 4: Coronal T1
From posterior (upper left) to anterior (lower right)
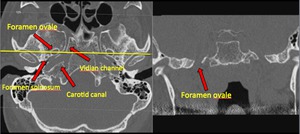
Fig. 5: Axial (left) and coronal (right) CT of the skull base. Bone window.
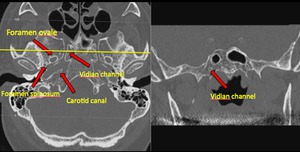
Fig. 6: Axial (left) and coronal (right) CT of the skull base. Bone window.
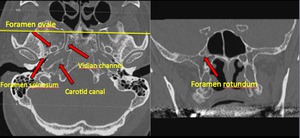
Fig. 7
More peripherally the three branches have their own course:
Ophtalmic (V1): superior orbital fissure >> travels superiorly and branches into lacrimal nerve; nasociliairy nerve and frontal nerve
Maxillary(V2): after coursing through the foramen rotundum,
it gives off small branches which extend caudally to the pterygopalatine fossa (important location of perineural spread) Note that this is in open contact with the inferior orbital fissure.
Most of the nerve travel ventrally through the infra-orbital canal.
Mandibular (V3): Caudally from the foramen ovale,
the nerve enters the posterior part of the masticator space.
It then splits into 2 branches: the lingual nerve and the inferior alveolar nerve which courses through the mandibular foramen and through a long canal in the mandibula and exits through the mental foramen.
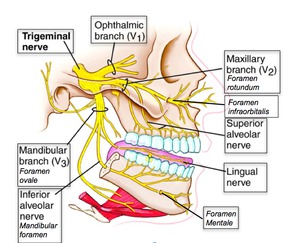
Fig. 8: Illustration of the branches of the trigeminal nerve.
References: http://msk-anatomy.blogspot.nl
Pterygopalatine fossa:
This fossa deserves special mention because of the extensive routes of spread via this site:
- Through the vidian channel to the facial nerve
- Through the inferior orbital fissure into the orbit
- Through the sphenopalatine fossa into the nasal cavity
- Directly to the mandibular nerve an then intracranially through the foramen rotundum or the infraorbital nerve.
- Directly to the masticator space
Facial nerve:
After leaving the brainstem the facial nerve enters the internal auditory meatus and travels through the petrosal bone.
Is makes a sharp turn at the geniculate ganglion,
and after a short horizontal course in a posterior lateral orientation,
it courses downward through the stylomastoid foramen.
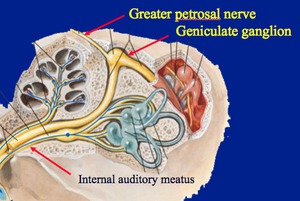
Fig. 9: Illustration of the facial nerve in the petrosal bone
References: Netter
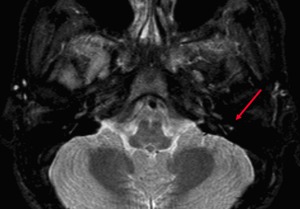
Fig. 11: Axial STIR
Patient with facial neuritis. The facial nerve is nicely depicted here, in the descending portion of the petrosal bone.
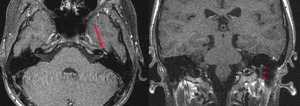
Fig. 10: Axial (left) and coronal (right)T1 post gadolinium.
Patient with facial neuritis. The geniculate ganglion is illustrated on the left. On the right the descending portion of the facial nerve is shown. Note the from the geniculate ganglion to the descending part the surrounding vasculature can enhance fysiologicaly, but symetrically.
The greater petrosal nerve coming from the geniculate ganglion,
travels through the vidian channel to the pterygopalatine fossa.
(see also figures: 6,
7 and 8)
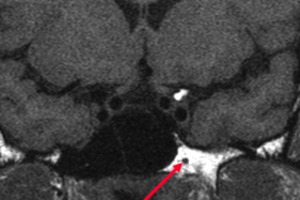
Fig. 12: Coronal T1
Vidian channel with the greater petrosal nerve, coming from the facial nerve and the deep petrosal nerve, coming from the sympathetic trunk. This is an important route of spread to and from the pterygopalatine fossa.
The facial nerve then gives off multiple branches which travel through the parotid gland to innervate multiple facial muscles.
Cavernous sinus:
Once the tumor has reached the cavernous sinus many other nerves can become involved and further spread can become extensive.
See figure:

Fig. 22: Cavernous sinus
References: Netter
QUIZ CASES
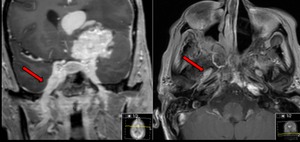
Fig. 13: Coronal (left) and axial (right) MR T1 post gadolinium.
Question 1: through which neuroforamen does this tumor spread,
and which nerve goes through this foramen?
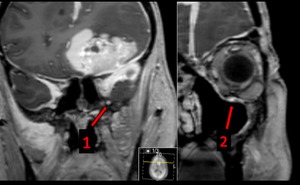
Fig. 14: Coronal T1 post gadolinium
The same patient as in figure 13. The right most image is more ventral.
Question 2:
Which foramen does arrow 1 point out? which nerve travels through this foramen?
Question 3:
Most part of the nerve from arrow one travels through arrow number two.
How is this nerve called?
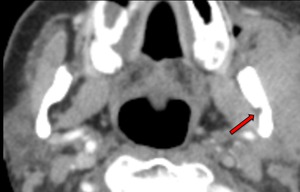
Fig. 15: Axial CT post contrast. Soft tissue window.
The arrow points out obliterated fat, notice the normal right side.
Question 4:
Which foramen is the arrow pointing out? How is the nerve called passing through it? From which nerve does it originate?
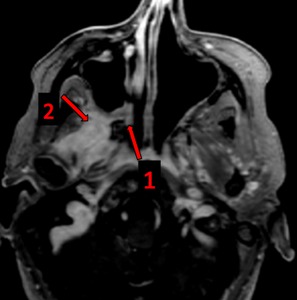
Fig. 16: Axial T1 post gadolinium.
Question 5:
How is the important anatomical site called at arrow 1?
Question 6:
To which space has the tumor spread (the primary tumor was located elsewhere) at arrow 2?
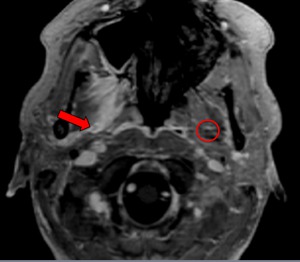
Fig. 17: Axial T1 post gadolinium
Case of figure 19. The nerve at the red arrow is at risk, the surrounding tissue enhances avidly. Notice the normal contralateral nerve (circle)
Question 7:
Which nerve in the masticator space is at risk for perineural spread?
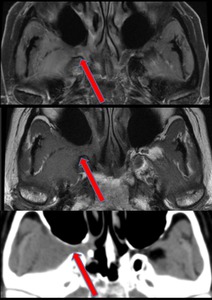
Fig. 18: From top to bottom: Axial MR T1; MR T1 post gadolinium; CT soft tissue window.
Another case with tumor infiltration in the pterygopalatine fossa, spreading directly to the masticator space. Notice the obliteration of the fatplanes compared to the other side.
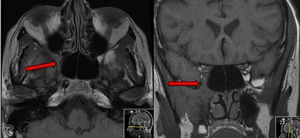
Fig. 19: MR axial T1 (left); coronal T1 (right)
Notice the tumor of figure 17 spreading upward.
Question 8:
To which fissure has the tumor spread ?

Fig. 20: MR coronal T1
Case of figure 17.
From the inferior orbital fissure the tumor has spread further upward and intracranially.
Question 9:
Which foramen is pointed out at number 1?
Question 10:
Which important anatomical location is obliterated intracranially?
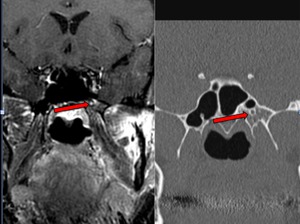
Fig. 21: MR coronal T1 post gadolinium (left) CT coronal bone window no contrast (right)
The nerve in the foramen which is pointed out enhances vividly. On CT there is a normal appearance.
Question 11:
Which foramen is pointed out? It is situated just medial and posterior to the foramen rotumdum.
Question 12:
Apart from the second division of the trigeminal nerve,
which other nerve is at risk and via which nerve does it spread?
Answers:
Question 1:
Foramen ovale; third division of the trigeminal nerve or mandibular nerve.
Question 2:
Foramen rotundum; second division of the trigeminal nerve or mandibular nerve.
Question 3:
Inferior orbital nerve.
Question 4:
Mandibular foramen; inferior alveolar nerve; from the thrid division of the trigeminal nerve
Question 5:
Fossa pterygopalatina
Question 6:
Masticator space.
Question 7:
The third division of the trigeminal nerve or mandibular nerve.
Question 8:
The inferior orbital fissure.
Question 9:
Foramen rotundum,
second division of the trigeminal nerve or mandibular nerve.
( see also question 2).
Question 10:
Cavernous sinus
Question 11:
Vidian channel
Question 12:
The facial nerve,
via the greater petrosal nerve
